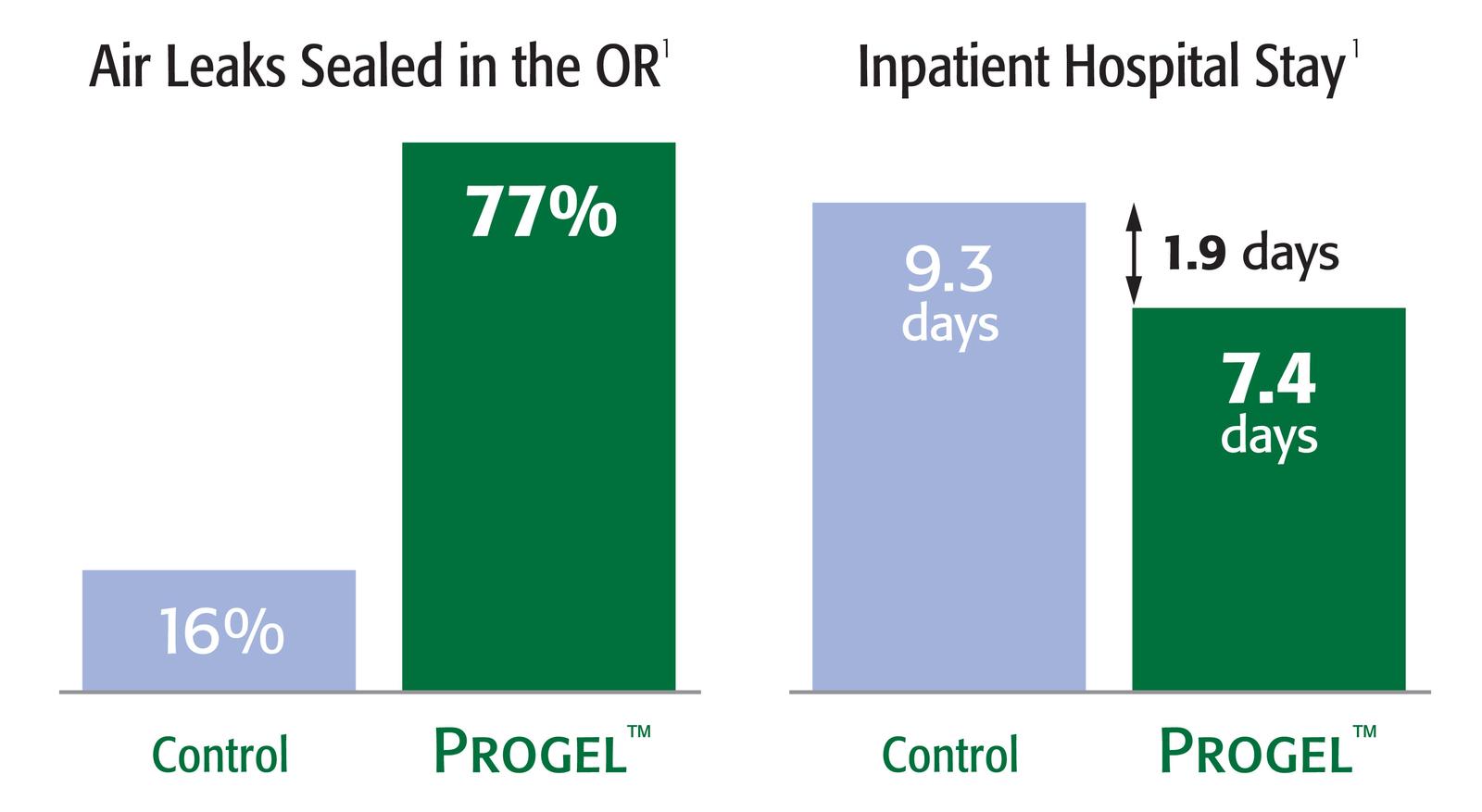
1. Allen, Mark S. et al, “Prospective Randomized Study Evaluating a Biodegradable Polymeric Sealant for Sealing Intraoperative Air Leaks That Occur During Pulmonary Resection” Annals of Thoracic Surgery 2004; 77:1792-1801. Pivotal study. Data on file.
2. Progel™ Pleural Air Leak Sealant Instructions for Use. M-00443. Davol Inc. Data on file.
3. Davol Inc. In Vitro Bench Testing. Data on File. In vitro test results may not correlate to clinical performance.
4. Brunelli et al. Predictors of prolonged air leak after pulmonary lobectomy. Ann Thorac Surg 2004; 77: 1205-1210. Based on the reported incidence of prolonged postoperative air leak.
5. Okereke, I, Murthy, SC, Alster, JM, Blackstone, EH, Rice, TW. Characterization and Importance of Air Leak After Lobectomy. Ann Thorac Surg 2005;79:1167-1173.
6. Estimated based on 4Q 2014 sales data and an estimate of 1.2 mL kits per procedure.
7. Prospective evaluation of biodegradable polymeric sealant for intraoperative air leaks Bernard J. Park1 *, John M. Snider2, Nathan R. Bates3, Stephen D. Cassivi4, G. Kimble Jett5, Joshua R. Sonett6 and Eric M. Toloza7
Intended Use / Indications For Use
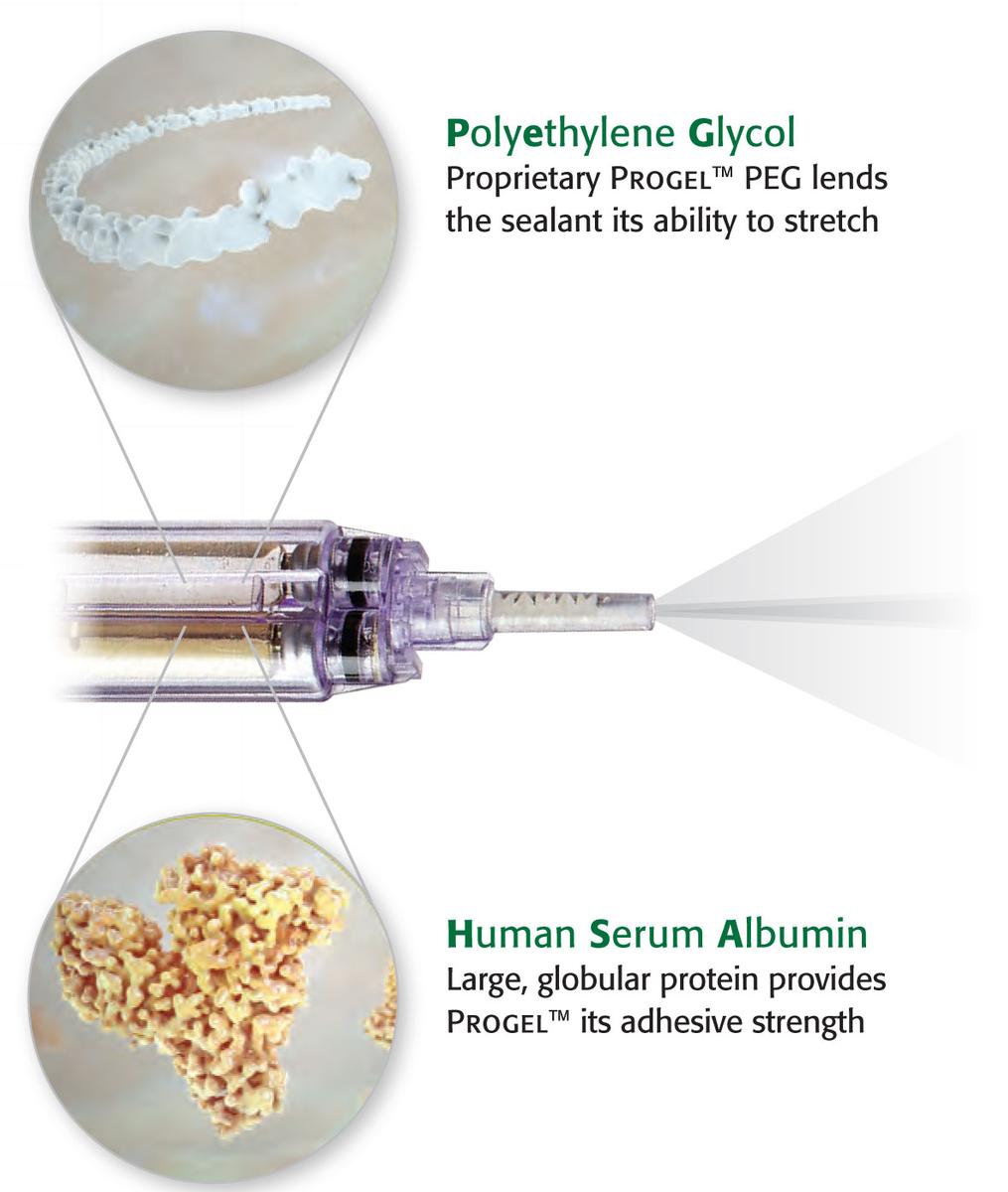
Progel™ Pleural Air Leak Sealant is a single use device intended for application to visceral pleura after standard visceral pleural closure with, for example, sutures or staples, of visible air leaks incurred during resection of lung parenchyma.
Contraindications
Do not use Progel™ PALS in patients who have a history of an allergic reaction to HSA or other device components. Do not use Progel™ PALS in patients who may have insufficient renal capacity for clearance of the Progel™ PALS PEG load. Do not apply Progel™ PALS on open or closed defects of main stem or lobar bronchi due to a possible increase in the incidence of bronchopleural fistulae, including patients undergoing pneumonectomy, any sleeve resection or bronchoplasty.
Warnings
Do not apply Progel™ PALS on oxidized regenerated cellulose, absorbable gelatin sponges or any other surface other than visceral pleura as adherence and intended outcome may be compromised.
Precautions
In the Post-approval study, the rate of post-operative pneumothorax was observed to be higher in patients treated with Progel™ PALS compared to control (standard-of-care), and the average duration of post-operative air leaks was not decreased when Progel™ PALS was used. In the post-approval study, the rate of post-operative pneumothorax was observed to be higher in patients treated with Progel™ PALS compared to control (standard-of-care), and 44% of Progel™ PALS subjects’ air leaks occurred when standard-of-care management techniques were not used. Progel™ is intended to be used only as an adjunct to standard of care management of intra-operative pleural air leaks. The safety and effectiveness of Progel™ PALS has not been established in the following: Patients less than 18 years of age; pregnant or nursing women; as a stand-alone therapy for intra-operative air leaks; contaminated or dirty pulmonary resection cases; the presence of an active infection; the presence of other sealants, hemostatic devices or products other than sutures and staples used in standard visceral pleural closure; visceral pleural air leak due to spontaneous pneumothorax, any non-resective pulmonary tissue trauma or malignancy, as well as congenital or acquired functional or anatomic defect; patients receiving Progel™ PALS in more than one application session (surgery) before and/or after resorption of Progel™ PALS that was applied in any previous surgical session; any area or tissue other than the visceral pleural surface as indicated; patients with forced expiratory volume in one second (FEV1) ≤ 40%, due to the small sample size of patients meeting this criteria in the original pivotal study. All five Progel™ PALS and four control patients with FEV1 ≤ 40% had postoperative air leak in the original pivotal study, whereas in patients with FEV1 > 40%, 59/93 Progel™ PALS patients (63.4%) and 45/53 control patients (84.9%) had postoperative air leak. See Section 7.9 Effectiveness: Primary Effectiveness Outcome in the Instructions for Use.
Adverse Events
There were 3 subjects in the Progel™ PALS group with AEs that were considered by the investigator to be possibly or probably related to the device. The AEs reported were: chest pain, constipation, gastroesophageal reflux, nausea, cough, dyspnea, pneumothorax, and subcutaneous emphysema. All were reported as a single occurrence in the Progel™ PALS group. Two of the AEs, dyspnea and chest pain, were reported as “severe” and “serious,” respectively and occurred in the same subject. All others were reported as mild (25%) or moderate (18.8%). In a clinical trial there were reports of renal dysfunction, urinary system disorders and deaths within the study population. None of these have been confirmed to be associated with Progel™. In a subsequent minimally invasive clinical trial there were no device related adverse events or unanticipated adverse events. The majority of AEs reported in this study were mild or moderate in severity. The majority of SAEs were pulmonary and expected events as part of a lung resection surgery. Two patients died during the course of the study, one due to cardiac arrest and another due to multi-system organ failure; neither were device related or unanticipated. The details of these clinical trial adverse events can be reviewed in the IFU supplied with the product and also available at http://www.bd.com
Caution: Federal (USA) law restricts this device to sale by or on order of a licensed physician or properly licensed practitioner.