IOH is a risk for all surgical patients
Despite overwhelming evidence associating intraoperative hypotension with poor outcomes, its prevalence remains high across surgical patient populations.
Even brief episodes of intraoperative hypotension (IOH) may lead to lasting harm

IOH is a serious public health issue.1
When blood pressure drops, risk rises
Intraoperative hypotension (IOH) is a frequent side effect of general anesthesia and is associated with increased risk of unfavorable outcomes for the patient.2-3 IOH is often a late-stage indicator of hemodynamic instability4 and is a serious risk factor that, when left unmanaged, can lead to sev ere complications.
Though IOH is common in non-cardiac surgical patients, numerous studies indicate that it is strongly associated with increased risk of myocardial injury after non-cardiac surgery (MINS), acute kidney injury (AKI) and mortality.2,5,6 The risks associated with IOH increase with the severity of hypotension.1,2

IOH is common and the consequences may be severe.
IOH is a risk for all surgical patients
Despite overwhelming evidence associating intraoperative hypotension with poor outcomes, its prevalence remains high across surgical patient populations.
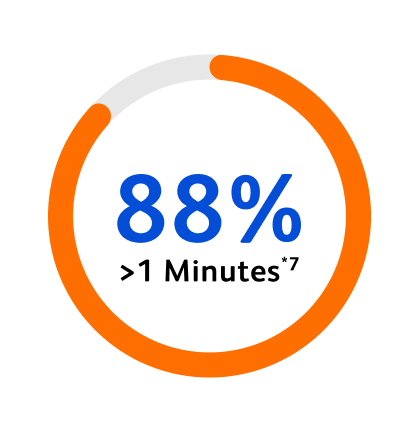
88% of non-cardiac surgery patients experience intraoperative hypotension for at least one minute.*7
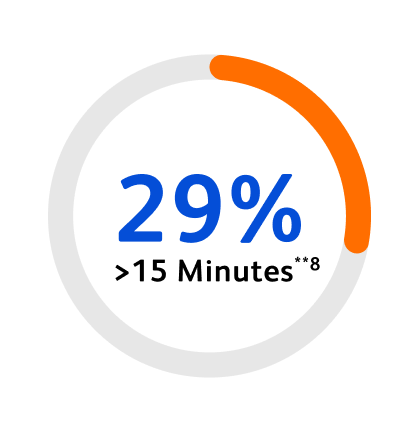
29% of patients experience IOH for at least 15 minutes in community anesthesia practices — where patients are typically considered low risk.**8
*Hypotension defined as MAP <65 mmHg for at least 1 min.
**In an observational study of 127,095 patients undergoing non-emergency, non-cardiac surgery in community anesthesia practices where hypotension is defined as MAP <65mmHg.
Even low-risk surgical patients may face serious consequences.
Injury is a function of intraoperative hypotension severity and duration.1
Numerous studies show that intraoperative hypotension is strongly associated with risk of end-organ injury – including myocardial injury after non-cardiac surgery (MINS), acute kidney injury (AKI) and delirium – as well as mortality.2-5

Exposure to lower MAPs is associated with increased risk of myocardial injury after non-cardiac surgery (MINS) and 30-day mortality.3,5

AKI is not only associated with poor outcomes and increased length of stay, but can also increase hospitalization costs ranging from $9,146 to $49,320.6

Patients typically considered lower risk are still susceptible to the adverse complications associated with IOH, including younger patients (18-39), patients with lower ASA physical status (ASA II), and patients undergoing shorter procedures.4,8,9,12

In a multicenter retrospective study of over 300,000 non-cardiac surgeries, there was no apparent safe amount of intraoperative hypotension.4
Depth and duration matter
Hypotension is not only common—non-cardiac surgical patients are also experiencing significant amounts. The depth and duration of hypotension directly correlates with the level of patient harm, making early detection and intervention essential.


*In an observational study where hypotension was defined as MAP <65 mmHg for ≥15 cumulative minutes.
Explore the research
For a review of the associations between IOH and risk of adverse clinical outcomes, see the list of published studies below.

Intraoperative hypotension is a modifiable risk factor that can, and needs to, be reduced.4,7,10
Hemodynamic instability is complex, and relying solely on blood pressure measurements can lead to missed warning signs or inappropriate treatments.
The Anesthesia Patient Safety Foundation has identified hemodynamic instability as a critical patient safety issue, emphasizing the need for proactive management to prevent harm.11

Blood pressure is the most widely used surrogate for hemodynamic instability in the perioperative period, but blood pressure alone does not reflect perfusion. By the time hypotension occurs, perfusion is often compromised.

Evidence shows that only 50% of episodes of hemodynamic instability solely require a vasopressor12—making it imperative to identify and treat the root cause for each individual patient.

Given the variability of underlying causes of intraoperative hypotension across patients, targeted, personalized treatment—guided by continuous advanced hemodynamic monitoring—is essential.
What if you could predict and prevent hypotension?
What if you could identify the potential root cause and intervene sooner?

Unlock the power of predictive care with Acumen HPI™ Software.
Acumen Hypotension Prediction Index™ (HPI™) Software provides earlier warnings, deeper insights, and more time to act, helping you stay ahead of hemodynamic instability. With advanced predictive intelligence, it’s a smarter way to monitor and personalize care for your patient’s needs.
The EU HYPROTECT study demonstrated that patients monitored with Acumen HPI™ Software experienced a low incidence, duration and severity of hypotension.*1
Low incidence of hypotension
41% of patients avoided hypotension when monitored with Acumen HPI™ Software, compared to 12% of patients in another large multicenter study where Acumen HPI™ Software was not used. *1,2
Brief duration of hypotension
Patients in this study experienced approximately 2 minutes of hypotension, or 1% of surgery time, compared with 28 minutes in another large multicenter study where Acumen HPI™ Software was not used.*1,2
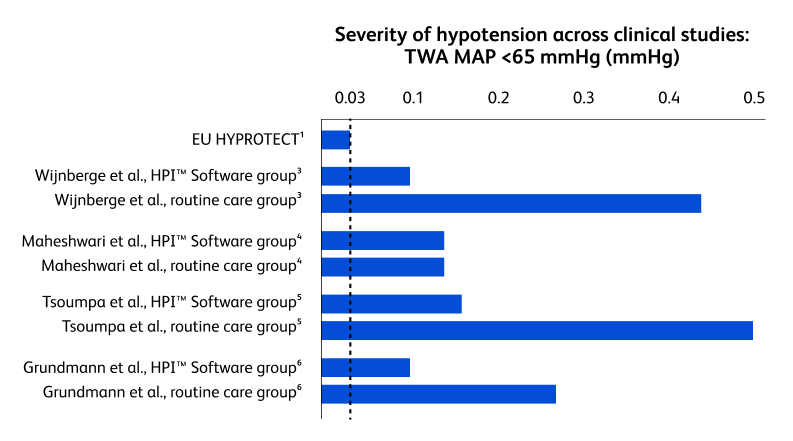
Low severity of hypotension
Patients monitored with Acumen HPI™ Software experienced a very low TWA MAP <65 mmHg at 0.03. The TWA MAP <60 mmHg was 0.*1
*Multicenter, prospective, observational study of patients across 5 EU countries monitored with Acumen IQ™ Arterial Line Sensor where hypotension was defined as >1 min below MAP 65 mmHg
Kouz K, Garcia MIM, Cerutti E, et al. Intraoperative hypotension when using hypotension prediction index software during major noncardiac surgery: A European multicentre prospective observational registry (EU HYPROTECT). BJA Open. 2023;6:100140.
Shah N, Mentz G, Kheterpal S. The incidence of intraoperative hypotension in moderate to high risk patients undergoing non-cardiac surgery: A retrospective multicenter observational analysis. J Clin Anesth. 2020;66:1-12.
Wijnberge M, Geerts BF, Hol L, et al. Effect of a machine learning-derived early warning system for intraoperative hypotension vs standard care on depth and duration of intraoperative hypotension during elective noncardiac surgery: the HYPE randomized clinical trial. JAMA. 2020;323(11):1052-1060.
Maheshwari K, Shimada T, Yang D, et al. Hypotension Prediction Index for prevention of hypotension during moderate- to high-risk noncardiac surgery. Anesthesiology. 2020;133(6):1214-1222.
Tsoumpa M, Kyttari A, Matiatou S, et al. The use of the Hypotension Prediction Index integrated in an algorithm of goal-directed hemodynamic treatment during moderate- and high-risk surgery. J Clin Med. 2021;10(24):5884.
Grundmann CD, Wischermann JM, Fassbender P, et al. Hemodynamic monitoring with Hypotension Prediction Index versus arterial waveform analysis alone and incidence of perioperative hypotension. Acta Anaesthesiol Scand. 2021;65(10):1404-1412.
CAUTION: Federal (United States) law restricts this device to sale by or on the order of a physician.
See instructions for use for full prescribing information, including indications, contraindications, warnings, precautions and adverse events.