




*As of April 2026 in the U.S. market
1 The Venovo™ Venous Stent System was studied in the global VERNACULAR clinical trial, which was a prospective, multi-center, non-randomized, single-arm study of 170 patients. The primary effectiveness endpoint of the study was primary patency (PP) at 12 months post-index procedure, defined as: freedom from target vessel revascularization and freedom from thrombus occlusion and stenosis >50% as measured by diagnostic ultrasound. Patients who received a Venovo™ Venous Stent had a weighted 12-month PP rate of 88.6%, demonstrating a statistically significant difference from a literature-derived performance goal (PG) of 74%. The primary safety endpoint was freedom from major adverse events (MAE) through 30 days post-index procedure. Freedom from MAE through 30 days was 93.5%, demonstrating a statistically significant difference from a literature-derived PG of 89%. There were no stent migrations associated with CEC-adjudicated events at the 30-day primary safety endpoint or through 36 months. Dake MD, O’Sullivan G, Shammas NW, et al. Three-year results from the Venovo venous stent study for the treatment of iliac and femoral vein obstruction. Cardiovasc Intervent Radiol. 2021;44(12):1918-1929. doi: 10.1007/s00270-021-02975-2
2 Foreshortening is calculated as the difference, represented as percentage, between the compressed stent length and expanded stent length at minimum/maximum oversize (1-3 mm). Across all sizes, foreshortening ranged from -4% to 10%, with a mean of 2.9% (values based on mathematical calculations). Bench tests may not be indicative of clinical performance. Different test methods may yield different results. Data on file, BD, Tempe, AZ.
Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, potential complications, adverse events and detailed safety information.
BD - 23533v6





* As of April 2026
1 The Venovo™ Venous Stent System was studied in the global VERNACULAR clinical trial, which was a prospective, multi-center, non-randomized, single-arm study of 170 patients. The primary effectiveness endpoint of the study was primary patency (PP) at 12 months post-index procedure, defined as: freedom from target vessel revascularization and freedom from thrombus occlusion and stenosis > 50% as measured by diagnostic ultrasound. Patients who received a Venovo™ Venous Stent had a weighted 12-month PP rate of 88.6%, demonstrating a statistically significant difference from a literature-derived performance goal (PG) of 74%. The primary safety endpoint was freedom from major adverse events (MAE) through 30 days post-index procedure. Freedom from MAE through 30 days was 93.5%, demonstrating a statistically significant difference from a literature-derived PG of 89%. There were no stent migrations associated with CEC-adjudicated events at the 30-day primary safety endpoint or through 36 months. Dake MD, O’Sullivan G, Shammas NW, et al. Three-year results from the Venovo venous stent study for the treatment of iliac and femoral vein obstruction. Cardiovasc Intervent Radiol. 2021;44(12):1918-1929. doi: 10.1007/s00270-021-02975-2
2 Simulated use data on file. BD, Tempe, AZ. Results may not be predictive of actual clinical outcomes. Different test methods may yield different results. Venovo™ Stent (14 mm x 100 mm, N=6), Medtronic Abre™ Stent (14 mm x 100 mm, N=6). The maximum pull-out force of an implant from a silicone tubing section at 1 mm oversizing and at an overlap length of 40 mm was measured. A higher pull-out force is interpreted as higher migration resistance. Venovo™ Stent demonstrated higher mean pull-out force (0.107 N/mm) compared to the Medtronic Abre™ Stent (0.095 N/mm).
3 Simulated use data on file. BD, Tempe, AZ. Results may not be predictive of actual clinical outcomes. Different test methods may yield different results. Venovo™ Stent (14 mm x 100 mm, N=6), Cook Zilver® Vena™ Stent (14 mm x 100 mm, N=6). The pull-out force of an implant from a silicone tubing section at the recommended minimum oversizing and at a defined overlap length was measured. A higher pull-out force is interpreted as higher migration resistance. Venovo™ Stent demonstrated higher mean pull-out force (0.110 N/mm) compared to the Cook Zilver® Vena™ Stent (0.038 N/mm).
BD - 23533v6
The VERNACULAR study results provide scientific evidence that the Venovo™ Venous Stent System is safe and effective for the treatment of symptomatic iliofemoral venous outflow obstruction.
To assess the safety and effectiveness of the Venovo™ Venous Stent for the treatment of iliofemoral venous occlusive disease.
170 subjects at 21 sites in the U.S., Europe, and Australia/New Zealand
Primary Patency: 84.0%
* Evaluated against literature derived performance goal of 74% for efficacy (p<.0001) and 89% for safety (p=.032)

Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, potential complications, adverse events and detailed safety information.
BD - 23533v4
Product Overview
Stent Wall Apposition
Venous Voices
Product Overview
Stent Wall Apposition
Venous Voices
Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, potential complications, adverse events and detailed safety information.
BD - 23533v6
Prospective, multi-center, non-randomized, single-arm;
Core lab & Data Safety Monitoring Board

*As of April 2026
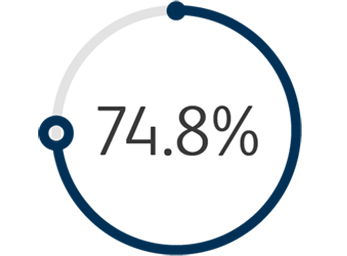
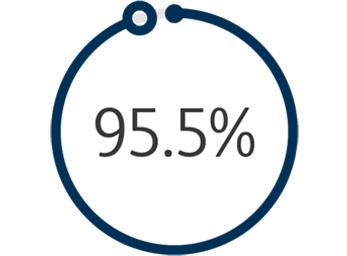
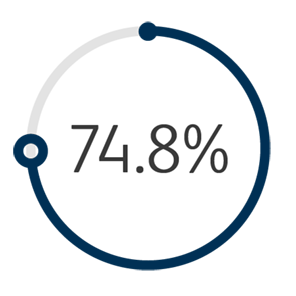
1 The Venovo™ Venous Stent System was studied in the global VERNACULAR clinical trial, which was a prospective, multi-center, non-randomized, single-arm study of 170 patients. The primary effectiveness endpoint of the study was primary patency (PP) at 12 months post-index procedure, defined as: freedom from TVR and freedom from thrombus occlusion and stenosis > 50% as measured by DUS. Patients who received a Venovo™ Venous Stent had a weighted PP rate of 88.6%, demonstrating a statistically significant difference from a literature-derived performance goal (PG) of 74%, with an 81.7% PP rate for subjects with post-thrombotic syndrome and 97.1% PP rate for subjects with non-thrombotic iliac vein lesions. The primary safety endpoint was freedom from major adverse events (MAE) through 30 days post-index procedure. Freedom from MAE was 93.5%, demonstrating a statistically significant difference from a literature-derived PG of 89%. There were no stent migrations associated with CEC-adjudicated events at the 30-day primary safety endpoint or through 36 months. Primary Patency by Kaplan-Meier estimates at 36 months are 84.0% for the total population (N=170), 74.8% for subjects with post-thrombotic syndrome (N=93) and 95.5% for subjects with non-thrombotic iliac vein lesions. Secondary endpoints included acute technical success, Quality of Life (QoL) assessment, Venous Clinical Severity Score (VCSS – Pain score) and stent fractures. Results demonstrated 100% acute technical success, defined as successful deployment of stent(s) to intended target with adequate lesion coverage as assessed by the Investigator at the time of the index procedure. TLR is defined as the first revascularization procedure in the target vessel(s) following the index procedure, as determined by an Independent Core Lab. The Freedom from TLR rate at 36 months was 88.1%. At the 36-month follow-up, the CIVIQ-20 assessment demonstrated a change from baseline in the total study population of -16.8 and, for the VCSS Pain score, a change from baseline in the total population of -1.8. Stents were evaluated at the 36-month follow-up for fracture analysis. An anteroposterior and lateral x-ray for each evaluated stent were sent to an independent core lab for analysis. 98 subjects’ x-rays were analyzed and no stent fractures were reported. Missing x-ray analyses were recorded as protocol deviations. Dake MD, O'Sullivan G, Shammas NW, et al. Three-year results from the Venovo Venous Stent study for the treatment of iliac and femoral vein obstruction. Cardiovasc Intervent Radiol. 2021;44(12):1918-1929. doi: 10.1007/s00270-021-02975-2
2 Evaluated against literature derived performance goal of 74% for efficacy (p<.0001) and 89% for safety (p=.0322)
Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, potential complications, adverse events and detailed safety information.
BD - 23533v6
Please consult Instructions for Use for product indications for use, contraindications, warnings, precautions, potential complications, adverse events and detailed safety information.
Our collection of literature on industries and our product offerings give you information you can use to continue striving for excellence.
Our eIFU portal allows you to search for a particular product's eIFU. Consult with your representative or check the product labeled IFU if no eIFU is found.
Safety and Risk Information
Indication for Use
The Venovo™ Venous Stent System is indicated for the treatment of symptomatic iliofemoral venous outflow obstruction.
Contraindications
The Venovo™ Venous Stent System is contraindicated for use in patients with a known hypersensitivity to nitinol (nickel-titanium) and tantalum, who cannot receive intraprocedural anti-coagulation therapy, or who are judged to have a lesion that prevents complete inflation of a balloon dilatation catheter or proper placement of the stent or the stent delivery system.
Warnings
The Venovo™ Venous Stent System is supplied sterile and is intended for single use only. Do not resterilize and/or reuse the device. Reuse, resterilization, reprocessing and/or repackaging may create a risk to the patient or user, may lead to infection or compromise the structural integrity and/or essential material and design characteristics of the device, which may lead to device failure, and/or lead to injury, illness, or death of the patient. Reusing this medical device bears the risk of cross-patient contamination as medical devices – particularly those with long and small lumina, joints, and/or crevices between components – are difficult or impossible to clean once body fluids or tissues with potential pyrogenic or microbial contamination have had contact with the medical device for an indeterminable period of time. The residue of biological material can promote the contamination of the device with pyrogens or microorganisms which may lead to infectious complications or death. Do not use in patients with total venous occlusion that cannot be dilated to allow passage of the guidewire. Do not use the device with contralateral access. Do not use if pouch is opened or damaged. Do not use the device after the “Use By” date specified on the label. Persons with allergic reactions to nitinol (nickel-titanium) alloy and/or tantalum may suffer an allergic response to this implant. Do not expose the delivery system to organic solvents, e.g., alcohol. The stent is not designed for repositioning or recapturing. Stenting across a major branch could cause difficulties during future diagnostic or therapeutic procedures. If a long lesion needs to be stented consider using the longest available stent rather than overlapping stents. If multiple stents are placed in an overlapping fashion, they should be of similar composition (i.e., nitinol). The long-term outcomes following repeat dilatation of endothelialized stents are unknown. The safety and effectiveness of this device for use in the arterial system have not been established.
Precautions
The device is intended for use by physicians who have received appropriate training. During system flushing, observe that saline exits at the catheter tip. The delivery system is not designed for use with power injection systems. Recrossing a partially or fully deployed stent with adjunct devices must be performed with caution. Prior to stent deployment, remove slack from the delivery system catheter outside the patient. If excessive force is felt during stent deployment, do not force the delivery system. Remove the delivery system and replace with a new unit. Store in a cool, dark, dry place. Do not attempt to break, damage, or disrupt the stent after placement.
Potential Complications and Adverse Events
Allergic/anaphylactic reaction; Amputation; Aneurysm; Arteriovenous fistula; Death related/unrelated to procedure; Dissection; Embolization; Extravasation; Fever; Hemorrhage/bleeding requiring a blood transfusion; Hematoma; Hypotension/hypertension; Incorrect positioning of the stent requiring further stenting or surgery; Intimal injury/dissection; Ischemia/infarction of tissue/organ; Local infection; Malposition (failure to deliver the stent to the intended site); Open surgical repair; Pain; Pulmonary embolism; Pseudoaneurysm; Renal failure; Respiratory arrest; Restenosis; Rupture; Septicemia/bacteremia; Stent Fracture; Stent Migration; Vasospasm; Venous occlusion/thrombosis/restenosis
Please consult product labels and instructions for use for indications, contraindications, hazards, warnings, and precautions.
BD, the BD logo, Bard, and Venovo are trademarks of Becton, Dickinson and Company or its affiliates. © 2020 BD. All rights reserved. Bard Peripheral Vascular, Inc. | 1 800 321 4254 | www.bardpv.com | 1625 W. 3rd Street Tempe, AZ 85281
BD-19558